Advanced Spinal Instrumentation Images
Welcome to Dr Khurana’s Advanced Spinal Instrumentation page.
Images shown here are with the permission of Dr Khurana’s patients, for educational purposes.
On this page, you will see:
- Anterior cervical reconstruction with artificial (mobile) discs and cage combinations;
- Percutaneous lumbar screws and rods placed accurately and minimally-invasively with the assistance of neuronavigation (“spinal GPS”) technology;
- Multilevel degenerative cervical spine reconstruction with 3 minimal-footprint lordotic interbody cages;
- Anterior lumbar interbody fusion (ALIF) at a relatively high level (L3/4) for severe degenerative disc disease and at multiple levels (L4/5 and L5/S1) for trauma, using minimal-footprint interbody cages and minimally invasive anterior surgical approaches.
Click any of the images below for a larger view; you can use the left and right arrow on the enlarged image viewer to scroll through all images on this page.
PATIENT 1 (below) – ANTERIOR CERVICAL SPINAL RECONSTRUCTION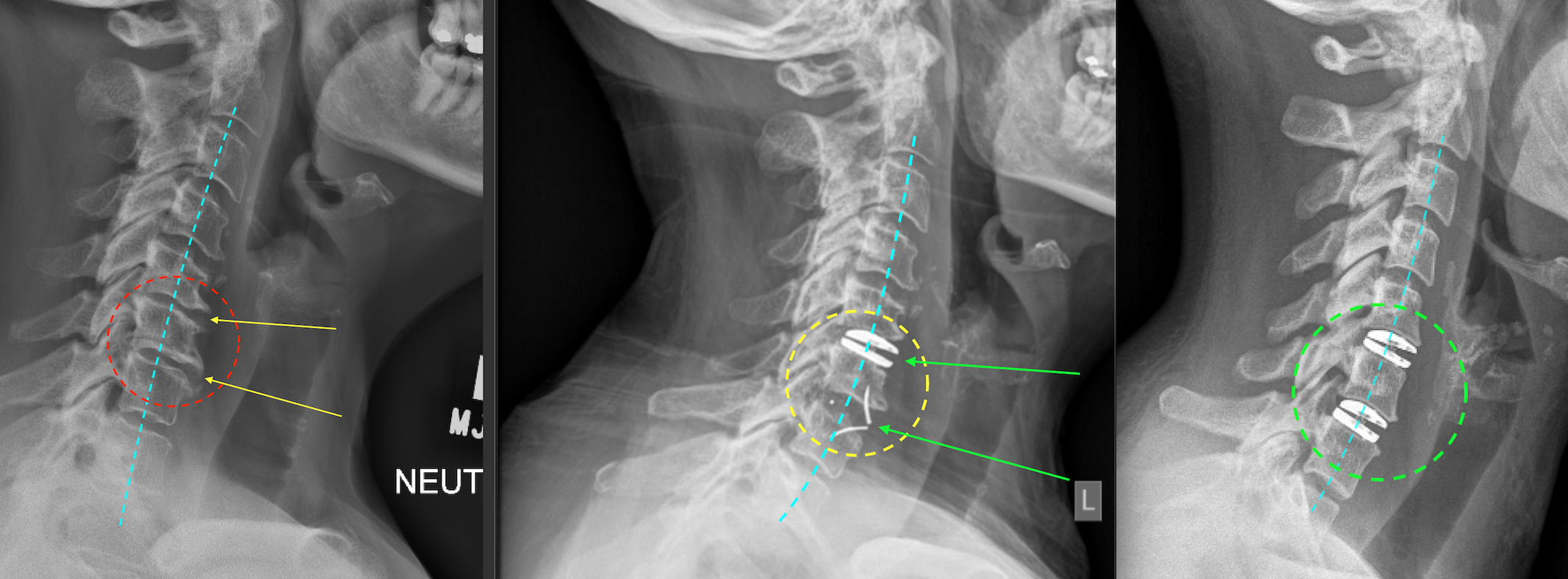
Panel above: “Worn out necks” with bone spurs (osteophytes), collapsed and dehydrated discs (desiccation), and poor neck shape (alordotic or reversed lordosis/kyphotic) can be structurally salvaged / “rejuvinated” by using a combination of prosthetics as shown above (artificial disc and cage, middle panel, or dual artificial discs, right panel). This can restore disc height and neck motion, decompress nerves and cord, and relieve pain and disability. I try to use as many artificial discs as I can, in the cervical and lumbar spine, i.e., whenever the anatomy permits.
PATIENT 2 (below) – LUMBAR SCOLIOSIS WITH NERVE ROOT COMPRESSION
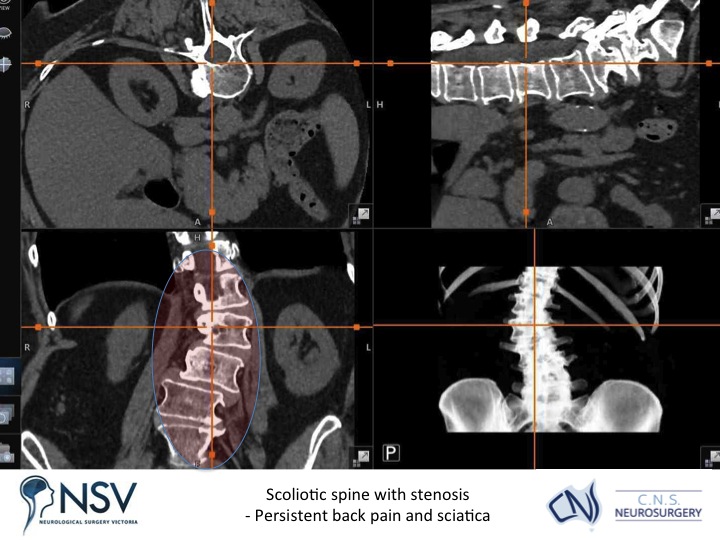
Panel above: This lady, with an abnormal curvature (scoliosis) of her lumbar spine, presented with longstanding, progressive severe back and leg pain.
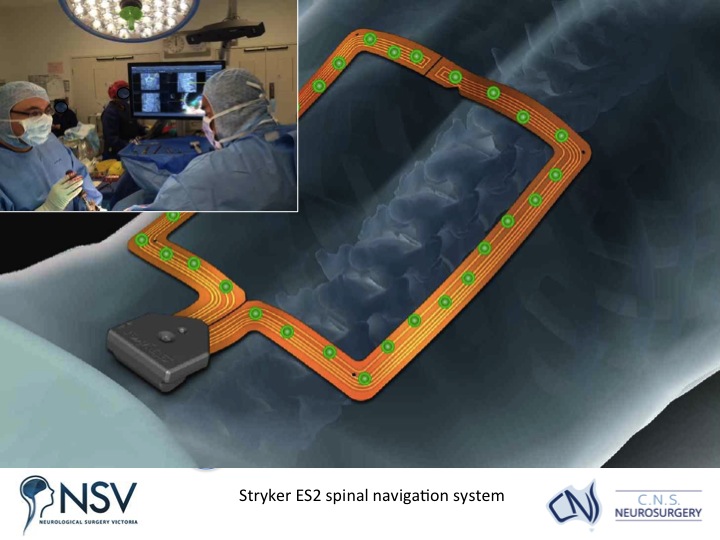
Panel above: The Stryker ES2 spinal navigation (“GPS-like”) system was used intraoperatively to gain an accurate multidimensional and interactive view of her spine as we operated.
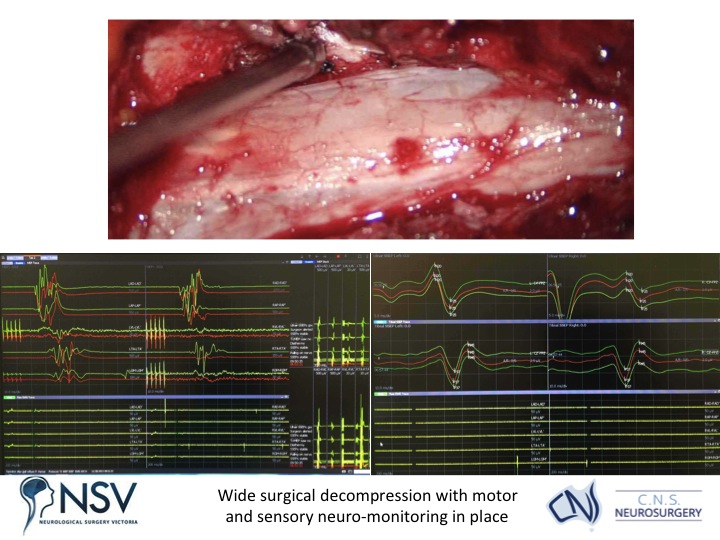
Panel above: An excellent decompression of the local tissues has been carried out, with view of the spinal (dural) tube and the previously severely compressed nerve root (at tip of the instrument) now decompressed via thorough rhizolysis. All of this while the patient’s neurological function was being monitored by electrodes in real-time as an added safety measure.
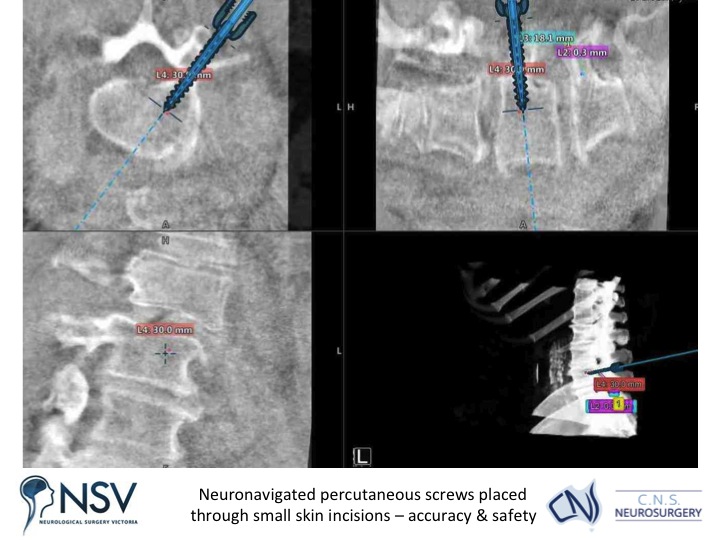
Panel above: The screw lengths and trajectories/vectors could all be planned prior to screw placement, and observed via the “GPS” system during placement. Again, all of this while the electrophysiologist in the room monitored the patient’s neurological function while she was anaesthetised.
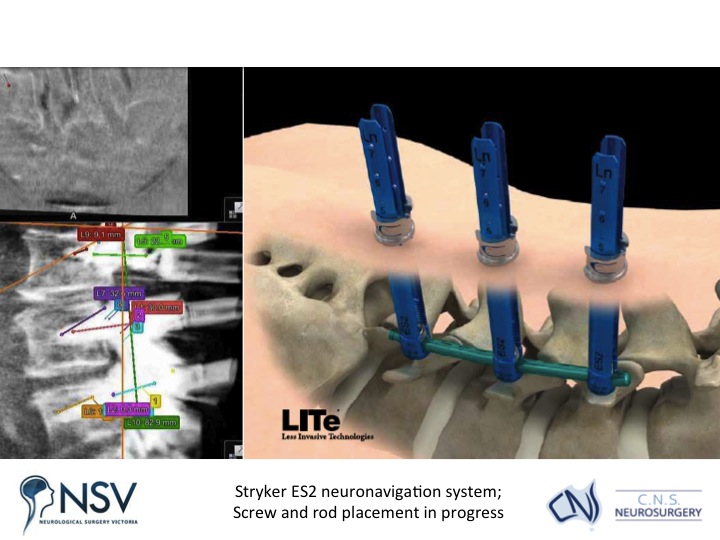
Panel above: A highly accurate placement of the screws and rods was achieved, the blue screw guides shown in the right image immediately above are removed at the end of the operation.
PATIENT 3 (below) – CERVICAL SPONDYLOSIS WITH REVERSED LORDOSIS AND IMPENDING CORD COMPRESSION
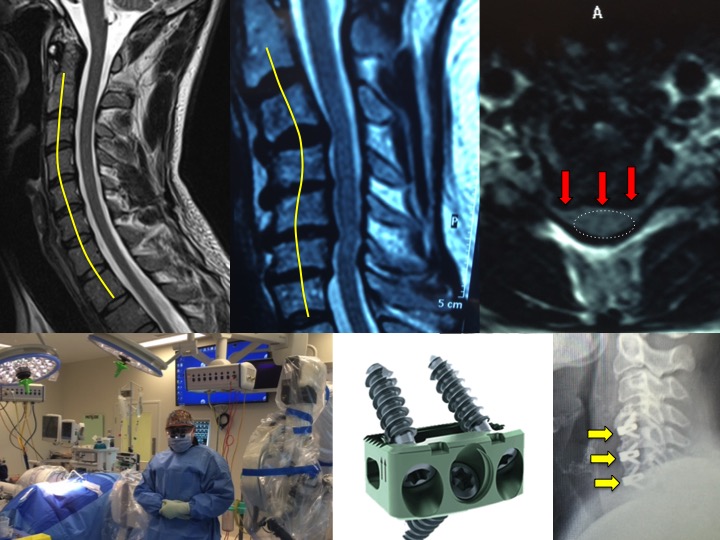
Panel above: This lady presented with severe neck and arm pain. The upper left image shows the normal cervical spinal curvature (“lordosis”). The upper middle image shows this particular patient’s curvature (“swan-neck” or “reversed lordosis”). Her substantial multi-level cervical disc disease and canal stenosis (upper right image, red arrows) are starting to compress her spinal cord. We surgically removed the three most diseased discs and in their place inserted three Chesapeake (lower middle and right images) minimal-footprint, lordotic cervical cages (approx. 17 mm wide), secured with a total of 9 titanium screws (approx. 14 mm length). The cages were filled centrally with iFactor bone-minerals to enhance fusion.
PATIENT 4 (below) – LUMBAR SPONDYLOSIS WITH SEVERE CHRONIC LOW BACK PAIN
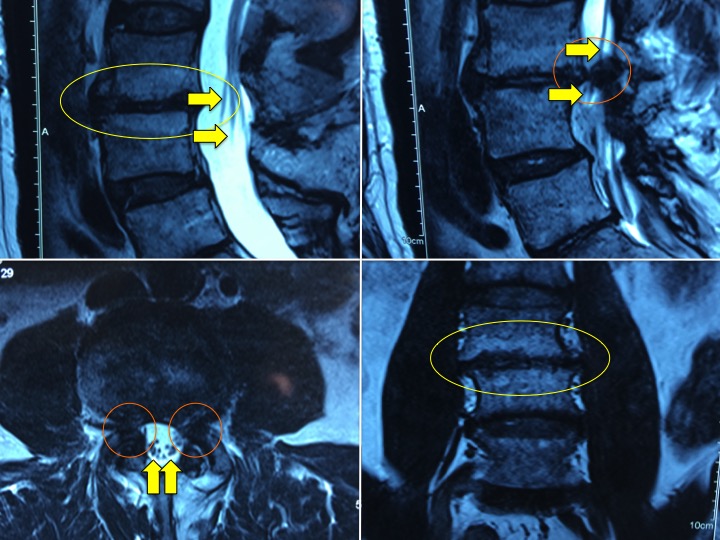
Panel above: This gentleman presented with long-standing, progressive lower back pain, with more frequent flare-ups of pain. The pre-operative MRI images show the effects of his degenerative L3/4 disc on the surrounding vertebral bodies (yellow circles, “Modic change”) and nerve roots (yellow arrows; stenosis).
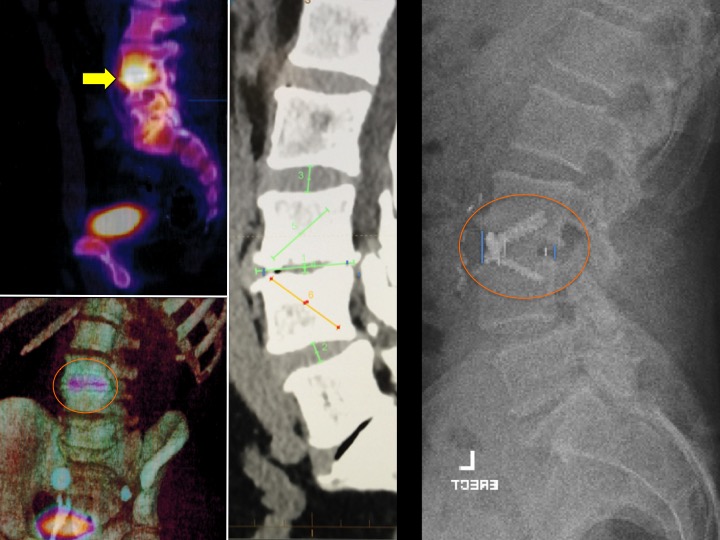
Panel above: The pre-operative CT SPECT scan (left 2 images) show the severely and actively affected level (L3/4; yellow arrow, yellow circle). The operation was planned (middle image) and carried out using a single Chesapeake (right image) minimal-footprint lordotic lumbar cage (36 mm wide), secured with a total of 3 titanium screws (25 mm length). The cage was placed following a minimally invasive access carried out by our gifted vascular surgeon. The small incision in the lower abdomen heals almost invisibly. The lumbar lordosis was restored by the appropriate customised cage.

Panel above: The patient wore this custom-fit brace when walking for the first 3 months postoperatively, in order to allow the fusion to mature. The lower right inset shows a Chesapeake lumbar cage device.
PATIENT 5 (below) – TRAUMATIC LUMBAR DISC DISEASE IN A YOUNG MAN (MOTOR ACCIDENT)
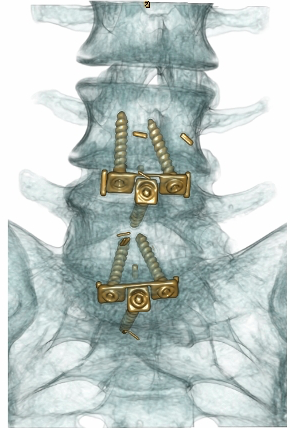
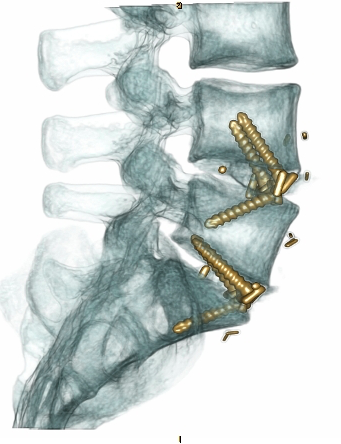
Panel above: The patient’s damaged lumbar discs which were causing chronic low back pain were successfully replaced with Chesapeake lumbar cages through a small anterior abdominal incision.