Hydrocephalus
Welcome to Dr Khurana’s Hydrocephalus page.
Images shown here are with the permission of Dr Khurana’s patients, for educational purposes.
-
- Image 1
-
- Image 2
Click images for larger view
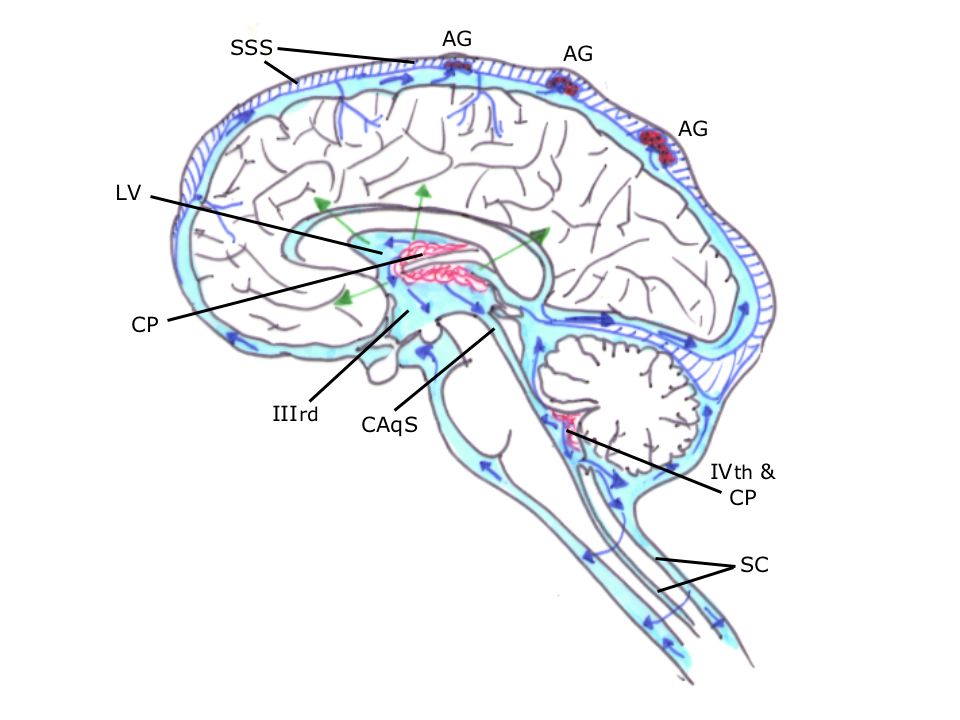
Hydrocephalus arises when there is an imbalance of cerebrospinal fluid (CSF) production versus its absorption.
Image 1 shows key sites of production, circulation and absorption of CSF in the central nervous system (CNS).
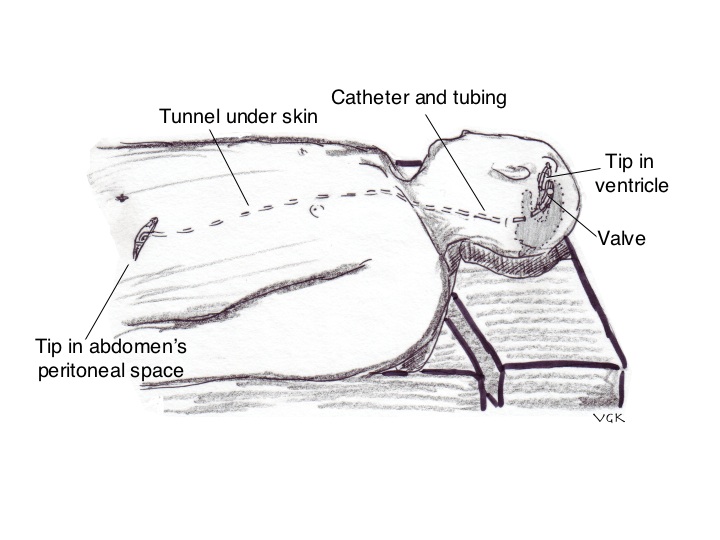
Image 2 is a diagram depicting a ventriculoperitoneal (VP) shunt placed to assist CSF drainage when there is too much CSF production compared with absorption; without the shunt, a gradual build up of CSF would occur resulting in the symptoms and signs of “raised intracranial pressure“.
-

- Image 3
-

- Image 4
-
- Image 5
-
- Image 6
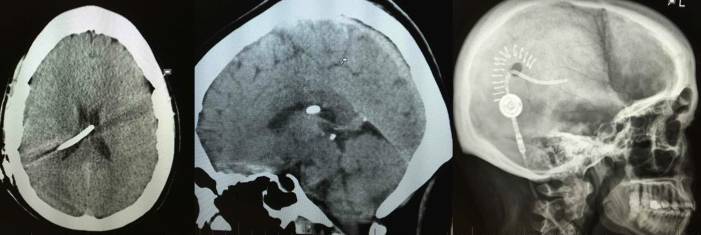
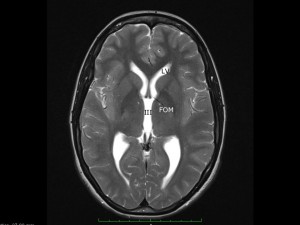
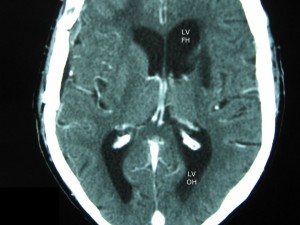
Hydrocephalus may be communicating (Images 5 & 6), where all ventricles communicate with one another, or it may be non-communicating / obstructive (Images 3 & 4), where one or more ventricles is/are obstructed, e.g., by a mass such as that shown above, an intraventricular tumour. In situations where obstructive hydrocephalus is diagnosed, the clinical goal is to relieve the symptoms definitively by treating the cause of the obstruction (in this particular patient, by removing the tumour).
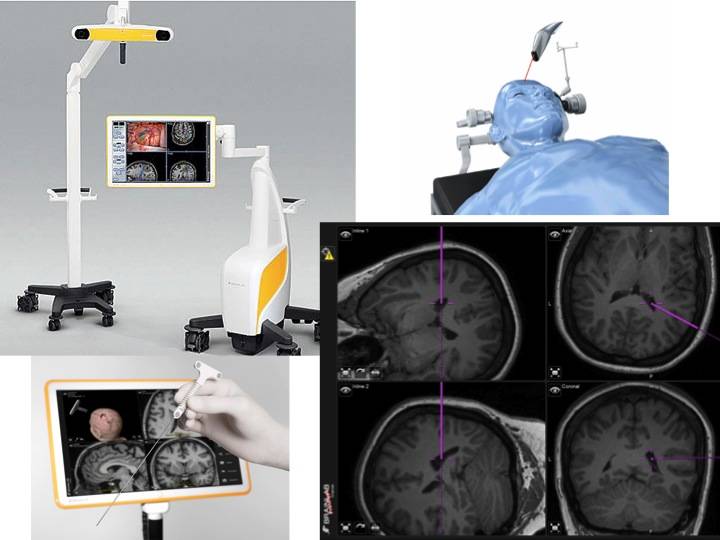
Brainlab neuronavigation systems (above). State-of-the-art, intuitive, real-time intraoperative “GPS”-like guidance.
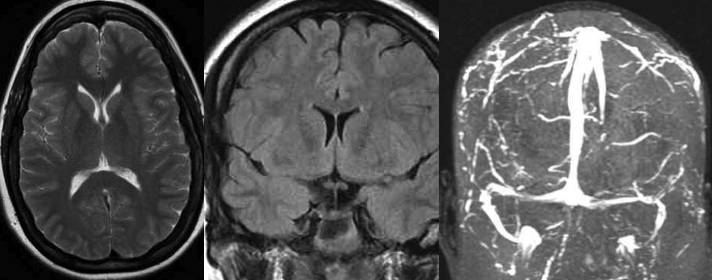
Pre-operative (Image 8): Idiopathic intracranial hypertension (MRI / MRV) – High intracranial pressure but small / narrow ventricles.
Patient presented with a diagnosis of “idiopathic intracranial hypertension” (aka “pseudotumor cerebri“), having had a number of lumbar punctures for CSF drainage, and was on Diamox. Treated definitively by stereotactic ventriculoperitoneal shunting (see below).