Carpal Tunnel
Welcome to Dr Khurana’s Carpal Tunnel page.
Images shown here are with the permission of Dr Khurana’s patients, for educational purposes.
Carpal Tunnel Syndrome is a relatively common condition, typically resulting from compression of the median nerve by thickened overlying tissues (especially the transverse carpal ligament / TCL) at the wrist. It may be associated with a number of conditions (e.g., diabetes, hypothyroidism, pregnancy, obesity, a ‘congenitally’ narrow tunnel, or trauma), but most occurences are without a specific cause. Occupational overusage/”RSI” has been implicated causally but remains controversial.
The key symptoms are progressive numbness and tingling (thumb, index, middle finger, and the adjacent surface of the ring finger), especially at night. Eventually if untreated, palmar atrophy (loss of tissue bulk) and weakness in aspects of the palmar grip can occur. While brace-splinting of the wrist may provide some temporary relief, if the symptoms recur or persist, and especially when verified by nerve conduction studies, then surgical decompression is reasonably undertaken.
{kind=link}
Carpal tunnel decompression is a straight forward “day-procedure” type operation, that can be done ‘open’ (a single small < 3.5 cm incision; when healed the incision is ‘hidden’ in a palmar crease — the location of the incision prior to surgery is shown in Image 1) or “endoscopically” (2 small incisions), and under either ‘general anaesthesia’, or (as Dr Khurana prefers) via a simple local anaesthetic ‘wrist block’ with some mild intravenous sedation.
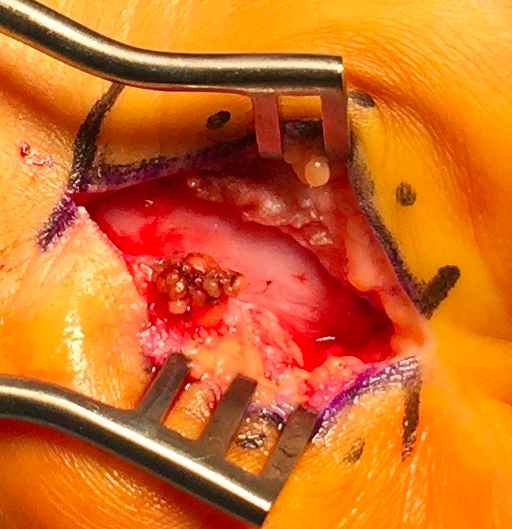
Our preferred theatre set-up is shown in Image 2, and the surgery requires only a few standard surgical instruments and the surgical part is usually done within 45 minutes. The thickened ligament is opened under direct visualisation (Image 3), and the median nerve is identified, protected and surgically decompressed (Image 4).
The incision is closed with some prolene sutures which are removed 10 days after surgery, and the arm is kept as elevated as possible for the first few postoperative days and ‘rested’ as much as possible for the first 4-6 weeks after surgery in order to optimise healing.
If the nerve conduction study results and the symptoms fit, the results of this minor but important procedure are typically excellent.
Click images for larger view.