CNS Neurosurgery | I’ve searched the world to find and use what I consider to be the best anterior spinal reconstruction prosthetics
I’ve searched the world to find and use what I consider to be the best anterior spinal reconstruction prosthetics
This ‘case study’ is a great example of how wonderful prosthetics can be used to reconstruct a neuro-compressive and increasingly painful cervical spine condition. These products are supported by scientific peer-reviewed published studies.
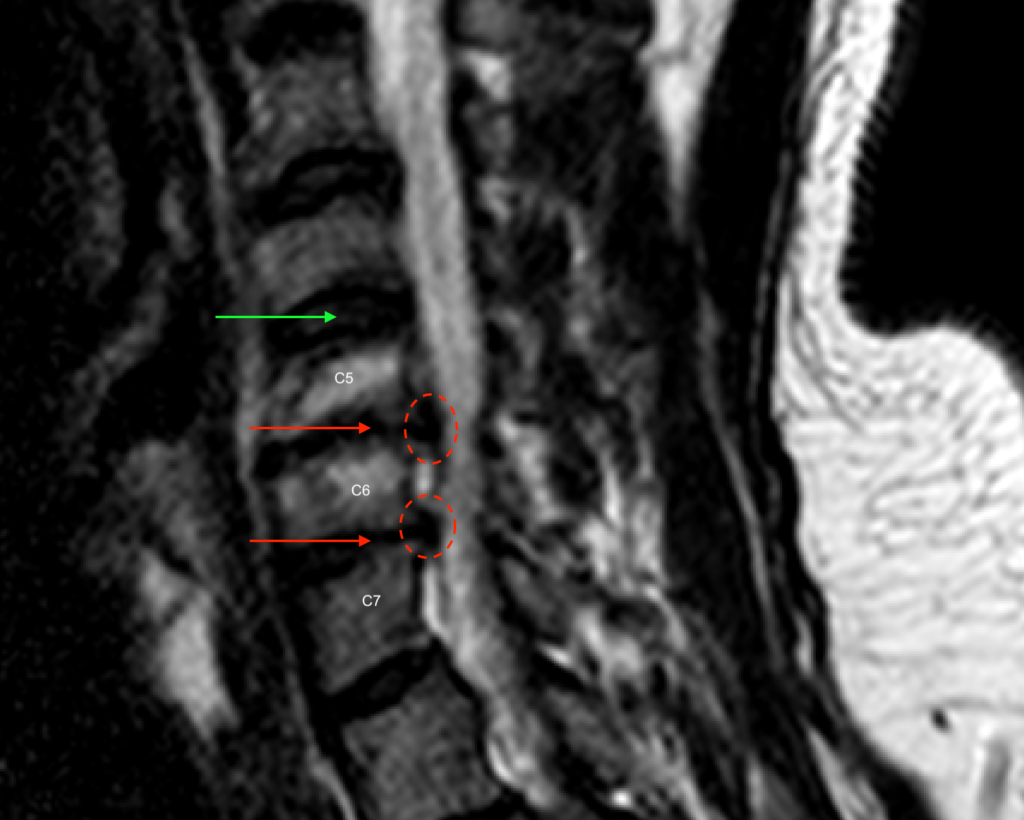
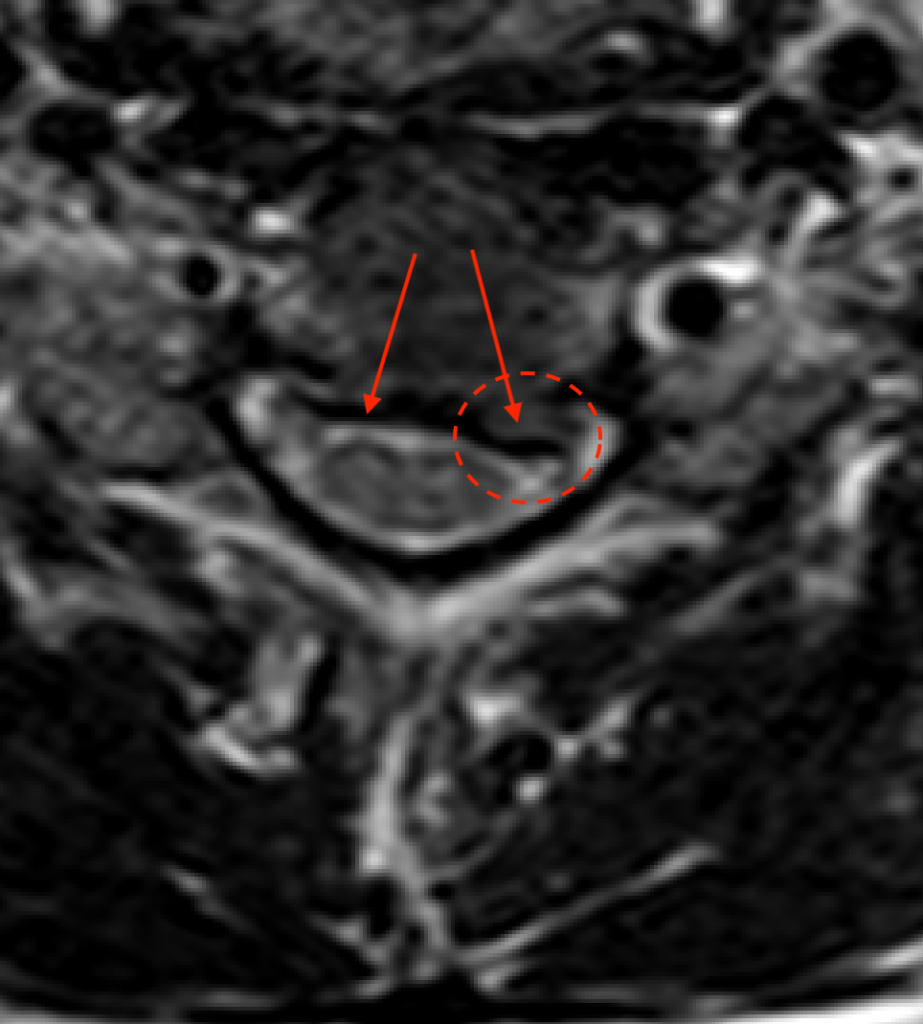
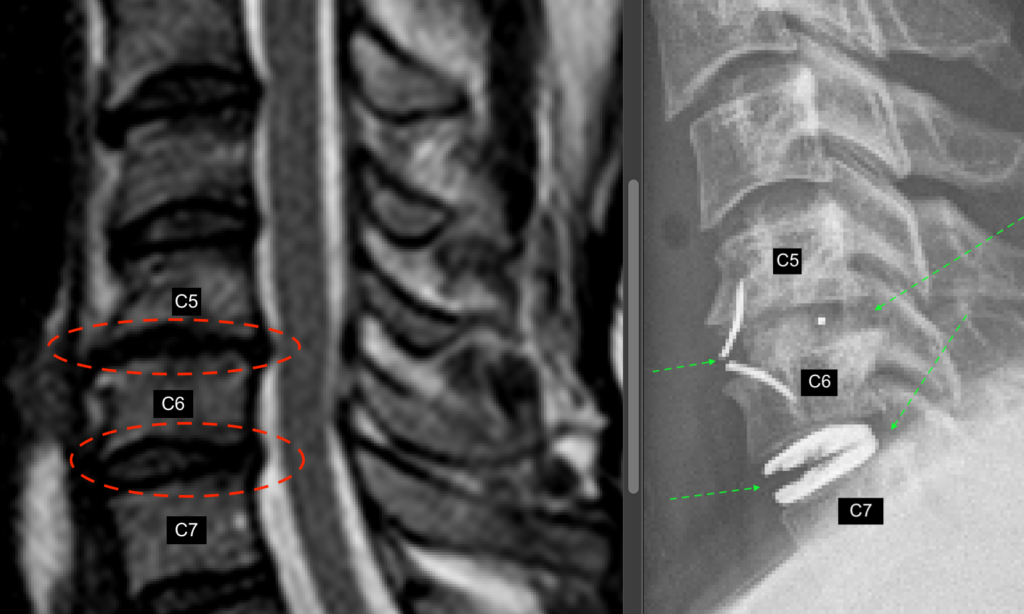
This nice man in his late-40s had presented with symptomatic cervical spondylosis. His pre-operative MRI of the cervical spine (the first two images below) showed collapse disc spaces (tips of red arrows) and calcified herniated discs (disc-osteophyte complexes; red dashed circles) at C5/6 and C6/7. A more normal looking disc space (at C4/5) is marked by the green arrow.
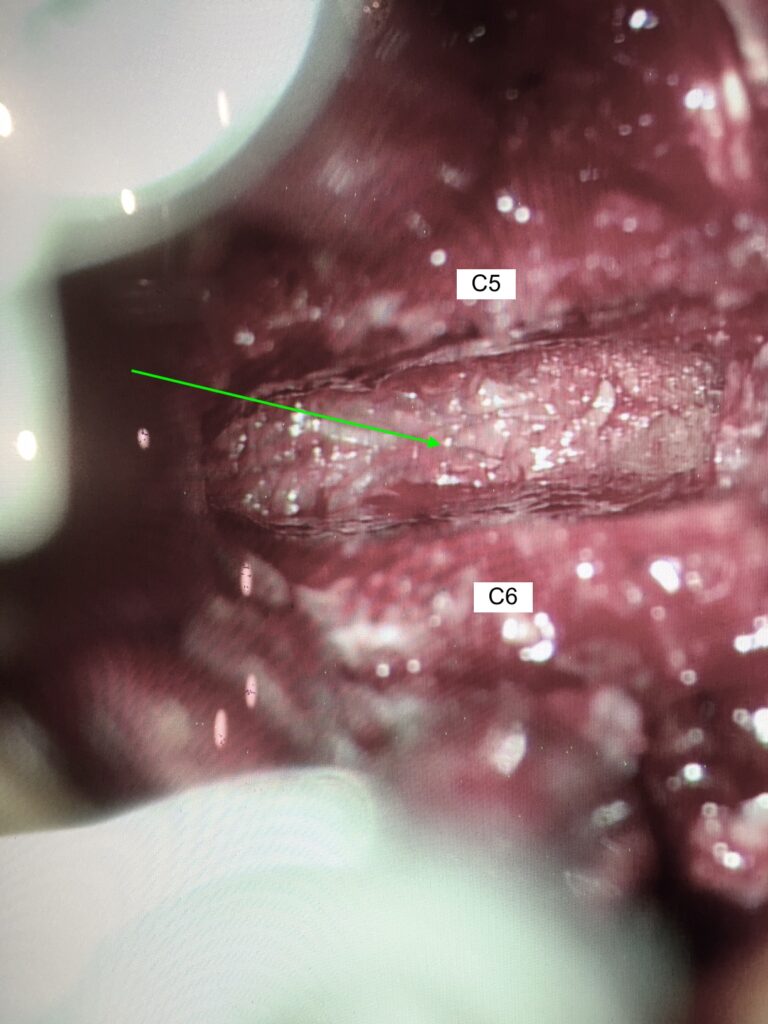
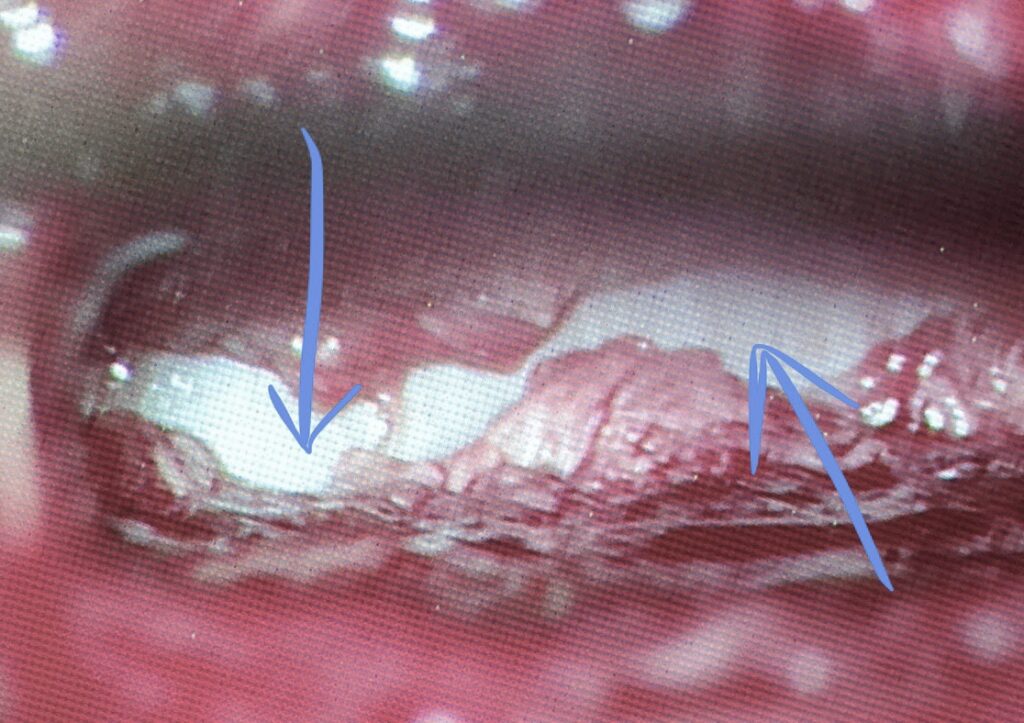
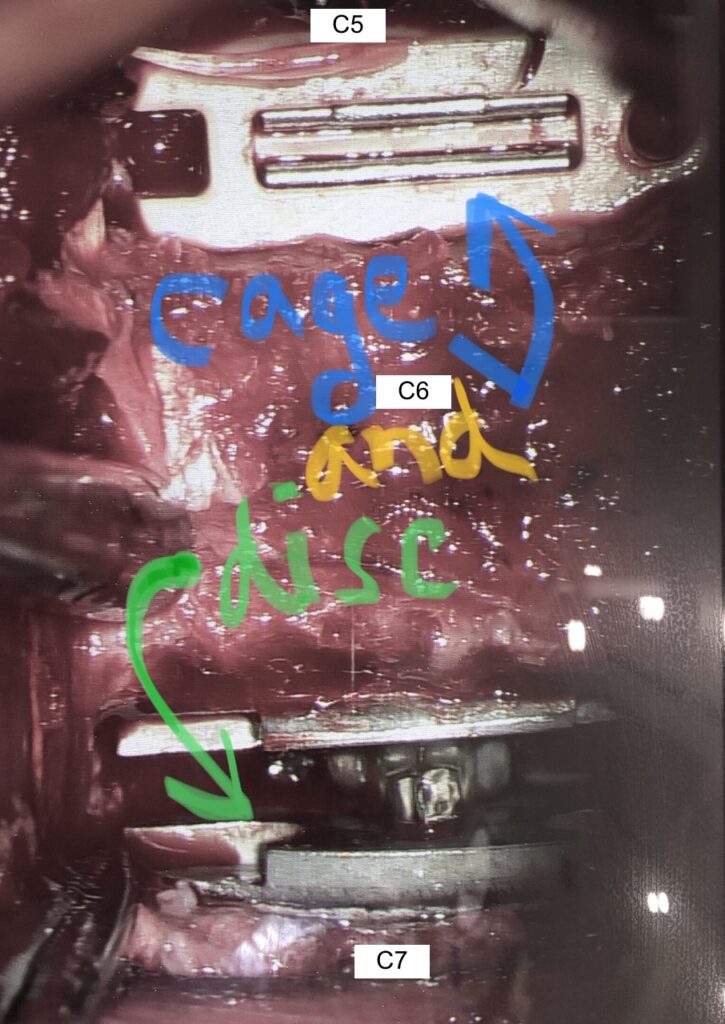
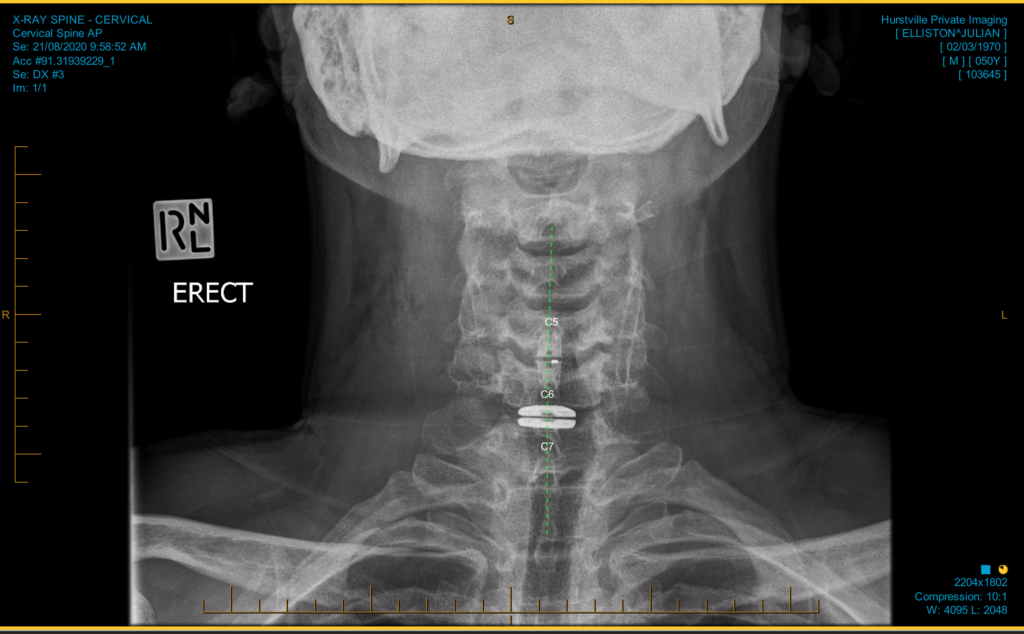
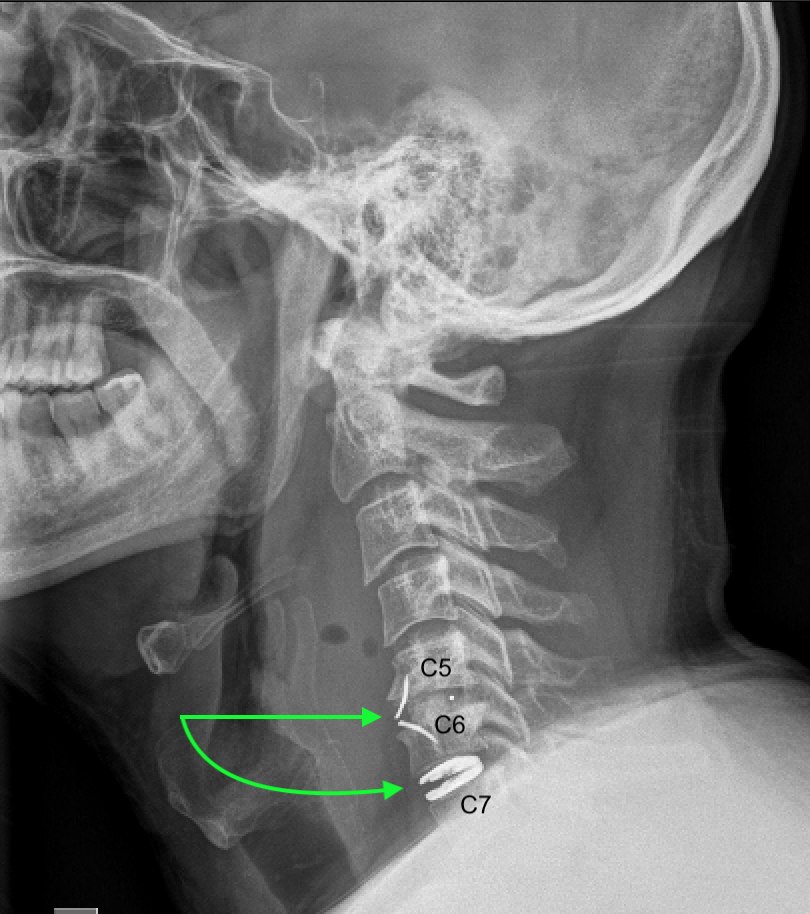
Pre-operative MRI (above) as described. Particularly note the “good” (C4/5) disc space versus the “bad” ones (C5/6 and C6/7). These are degenerative, like flat tyres. The white parts of the surrounding bones in C5 and C6 are like “tooth decay” called Modic change, occurring once the discs have lost their cushioning (advanced desiccation).You can see one of his disc-osteophyte spurs (in the red dashed circle) compressing the exiting nerve root and flattening the cervical cord.Via a small front neck incision, and under direct visualisation (illumination, magnification) of our Zeiss operating microscope, I removed the degenerative disc and then drilled out a lovely “mailbox” like space (green arrow) where the worn, collapsed, herniated disc once was.I then, with a micro-scalpel and tiny Kerrison rongeurs, opened up the posterior longitudinal ligament (PLL; the reddish yellow fibrous bands here) to expose the front of the cervical spinal cord (its white dural sheath seen here; tips of blue arrows). This key step allowed me to debulk more of the disc osteophyte spurs.I then put what I believe to be the two best prosthetics available for this operation. An ingeniously refined cage with a fusion core packed with special bone-forming compound (at C5/6; blue arrow), and a very special type of artificial mobile disc (at C6/7; green arrow). This is a “hybrid” reconstruction, with prosthetics chosen and tailored for the particular anatomical circumstance I encountered/expected. A beautiful result as shown on the AP cervical spine x-ray post-op. (I use X-rays as needed intraop., including during the device placement at each level).A beautiful post-op. lateral cervical spine X-ray result too. You can see the titanium parts (bright white here) of the prosthetics (gull-wing anchors for the cage at C5/6, and the artificial disc surfaces at C6/7). No bulky plates, no screws. Just sleek, elegant, functional and durable hardware.The pre-op. sagittal MRI is on the left, and the post-op. lateral X-ray is on the right. Notice how the reconstructed disc spaces are now large and normal again, like when this chap was much younger! Happy patient. Happy surgeon. He should continue to do well.< Back to blog