Microvascular decompression (MVD) for Trigeminal Neuralgia – Brainstem Microsurgery
These photographs show the surgical correction of a severe structural compression and deflection of the trigeminal nerve caused by an “offending” loop of the superior cerebellar artery.
(Click the link at the bottom of this page to learn more about trigeminal neuralgia and how it can be surgically treated if longstanding and unresolved by medical treatments)
The patient whose intra-operative images are shown below has had many years of severe trigeminal neuralgia affecting the whole of her right face (V1-V3 distributions).
IMAGE 1 (below): Look at how a loop of the “offending” superior cerebellar artery (yellow arrows) kinks and distorts the trigeminal nerve (blue arrows) across its V1-3 rootlets. This neurovascular “conflict” (i.e., direct pulsatile connection between the offending vessel and the nerve) causes trigeminal neuralgia.
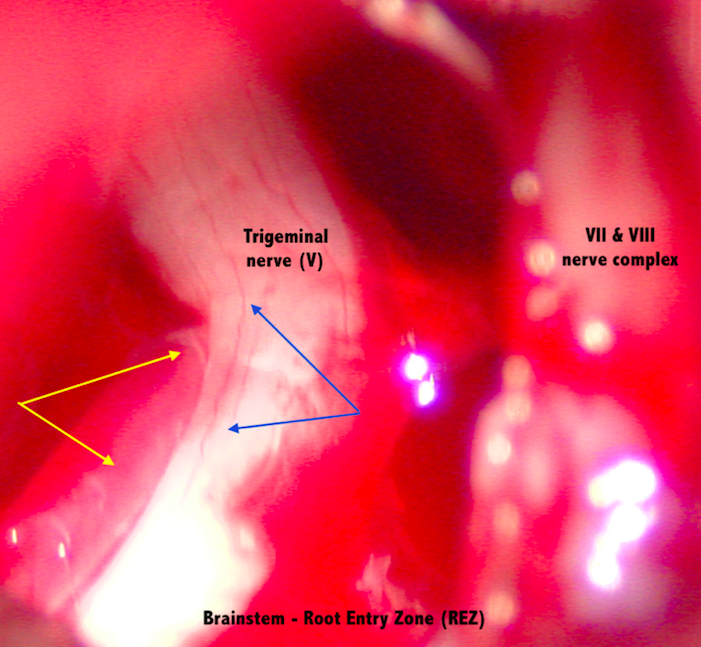
IMAGE 2 (below): Here I have moved the trigeminal nerve out of the way with a small titanium instrument called a Rhoton #6 microdissector; its tip is only 2mm (right hand side of image; that gives you an idea of how small these critical structures shown here are). You can now see the “offending” loop of artery (yellow arrows) better. The whitish shiny structure in the centre of the photograph draped across the upper part of the blood vessel loop is simply a thin curtain of natural “arachnoid” membrane. The curtain was microsurgically opened to allow the nerve and vessel to be mobilised (see Image 3).
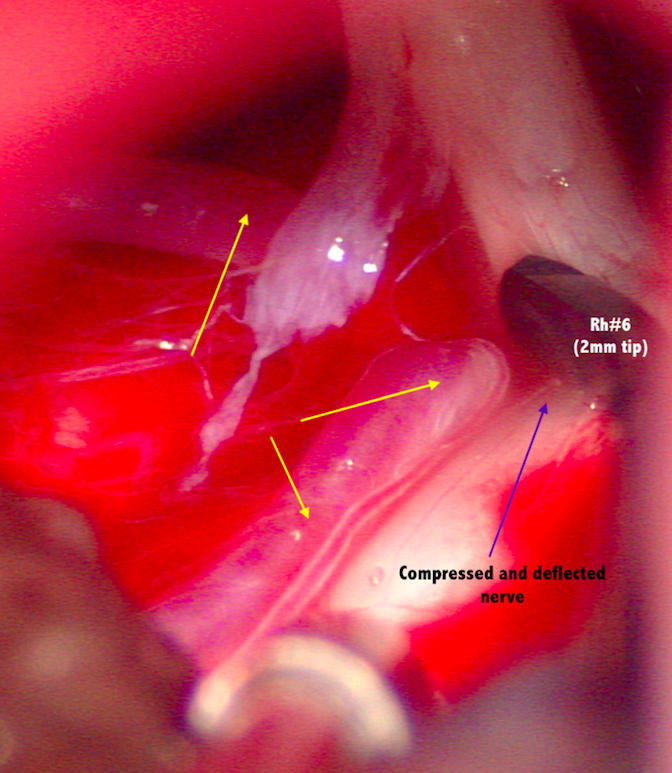
IMAGE 3 (below): After gently mobilising the artery away from the nerve, I have placed a cushion of PTFE/Teflon fibres between the offending blood vessel (yellow arrows) and the under surface of the trigeminal nerve (blue arrows). This arrangement was ‘bio-glued’ into place with two drops of Tisseal, a technique I learned from the MVD master surgeon, Dr Taka Fukushima.
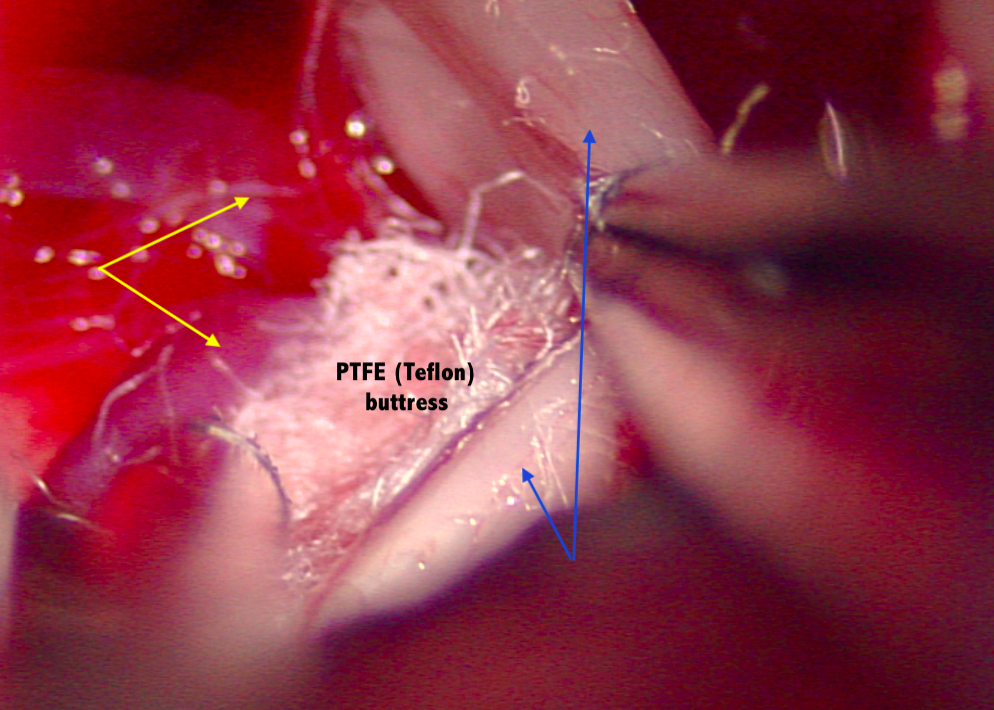
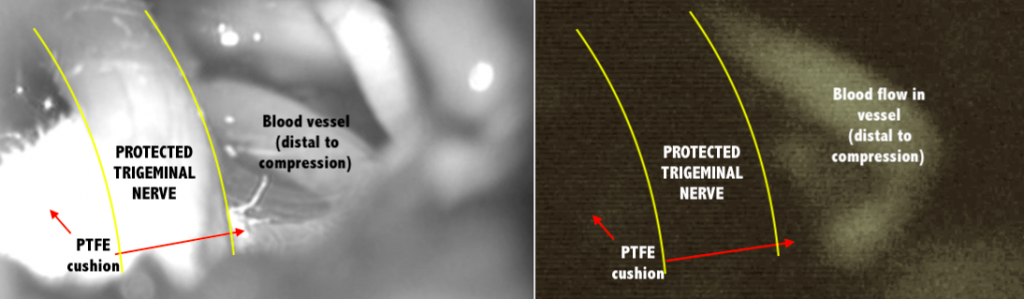
IMAGE 4 (below): At the end of the procedure, I carried out indocyanine green / ICG videoangiography to make sure the offending blood vessel’s blood flow was still present, and unaffected by the PTFE cushion that had been used to hold the vessel away from the nerve.
All of this was done with BrainLab neuro-navigation and a sophisticated fluorescence-enabled Leica operating microscope, and via a mini-craniotomy behind the right ear; the mini-craniotomy is the size of an Australian 10 cent coin!
To learn more, including with a demonstration video, CLICK HERE.
< Back to blog