Nice lumbar RANGE OF MOTION even following anterior + posterior prosthetic & instrumentation reconstruction
This otherwise healthy, active and working man presented with symptoms including persistent low back pain and bilateral leg radiating symptoms. They were substantially interfering with his quality of life. The L4/5 disc was “black” (desiccated, i.e., dehydrated and shrunken in height), as well as “slipped” (listhesed), from facet joint degeneration (degenerative spondylolisthesis).
The pre-operative key images, below, (Panels A & B) show this.
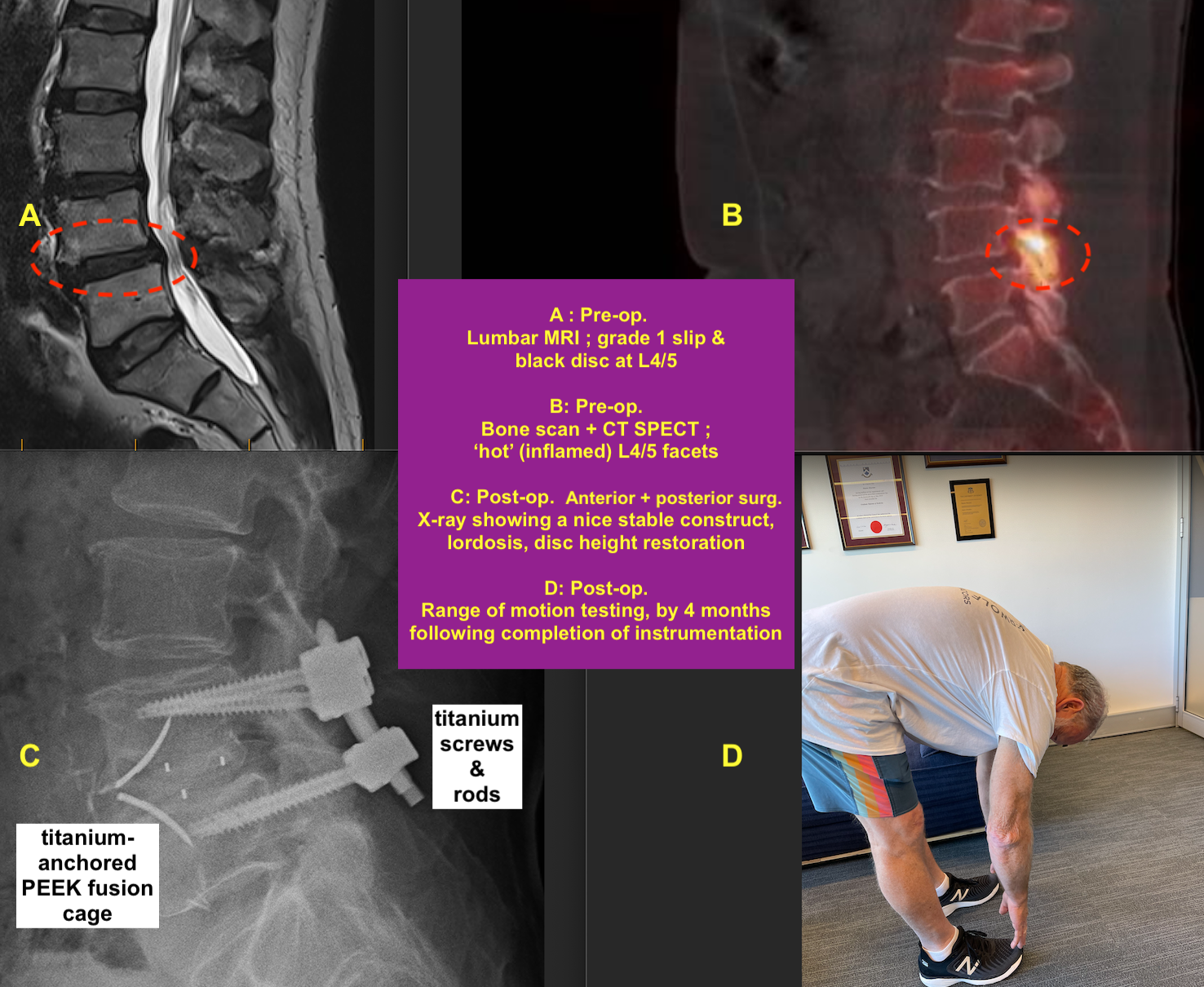
Anterior: ALIF – Anterior lumbar interbody fusion. Vertical abdominal incision, retroperitoneal approach via the vascular surgeon; robust anchored cage (PEEK body, titanium anchors, Allovance core).
Posterior: Decompression, followed by further instrumentation to optimise the construct and its stability. Posterior midline incision, stereotaxy-navigated procedure; real-time sensory and motor neuromonitoring; titanium transpedicular screws and interconnecting rods.
His post-operative range of motion in the lumbar spine remains excellent (Panel D, above) despite the rigid construct.
He is cheerful, active, and reports no back or leg symptoms now, and there is no sensory or motor deficit. I have provided my post-operative spinal health recommendations.
Post finalised 21-7-23
< Back to blog